Publisher's note: The author of this post is Jon Sanders, who is Director of Regulatory Studies for the John Locke Foundation.
North Carolina has one of the most aggressive Certificate of Need (CON) programs in the nation. A bipartisan bill introduced this week in the North Carolina House would loosen some of the CON reins.
House Bill 200, sponsored by Rep. Marilyn Avila (R-Wake) and co-sponsored by Rep. Jeff Colllins (R-Nash), Rep. Dan Bishop (R-Mecklenburg), and Rep. Mickey Michaux (D-Durham), would repeal portions of the state's CON regulations.
Carolina Journal
reports:
If passed, the legislation would exempt diagnostic centers, ambulatory surgical facilities, gastrointestinal endoscopy rooms, and psychiatric hospitals from certificate of need review. It also would prohibit the state medical facilities plan from limiting the number of operating rooms and gastrointestinal endoscopy rooms. ...
An ambulatory surgery center's "price differential from a hospital location is tremendous. It can be as much as 40 percent difference," Avila said. "It can be three times more in terms of price" to perform a procedure in a hospital than what an ambulatory surgery center would charge.
Regulating 25 services, the state's CON program is one of the country's most far-reaching:
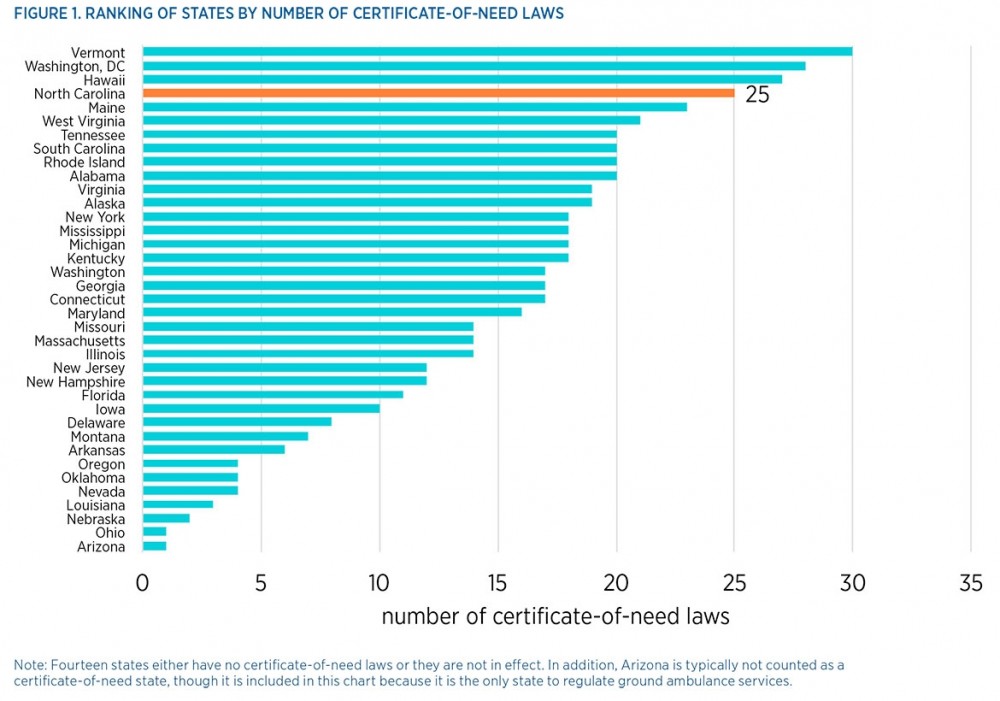
The chart (click for a bigger image) is from a
February 2015 study of North Carolina's CON program by researchers at the Mercatus Center of George Mason University. Researchers noted that "40 years of evidence demonstrate that these programs do not achieve their intended outcomes, but rather decrease the supply and availability of health care services by limiting entry and competition.
A 'remarkable consensus' in research literature
My
Carolina Cronyism report on North Carolina's CON regulations discussed that research consensus on CON, which was a federal mandate from 1974. Aimed at lowering health care costs, CON was repealed by Congress in 1987 after aggregate spending on health care had reached historic highs. Fourteen states have since repealed their CON programs.
Researcher Patrick McGinley surveyed the academic literature into CON laws and found a surprisingly uniform result: "In searching the scholarly journals, one cannot find a single article that asserts that CON laws succeed in lowering health care costs. CON 'has elicited
a remarkable evaluative consensus — that it does not work.'"
CON's failures go beyond making health care services costlier and more scarce, however. As I explained:
North Carolina's CON program negatively affects health care consumers and local communities, especially small towns and rural areas. The impact is more than just artificially higher prices. The elderly, the poor, people under time constraints (mothers, small business owners, etc.), and — especially! — people with emergency medical needs are better served by having medical services nearby.
Who benefits from keeping medical services more disparate and scarce? Existing hospitals and medical service providers, who reap the benefit of CON laws insulating them from competition. That benefit may not be unintentional, however — as East Carolina University researchers Ellen S. Campbell and Gary M. Fournier found, the states most likely to enact CON regulations "were those with a highly concentrated hospital industry and increasing competitive pressures," with hospitals largely favoring CON laws, which protect them from competition.
As things stand now, fewer than one-fourth (23 out of 100) of counties in North Carolina have more than one hospital. Seventeen counties still have no hospital.
Furthermore, North Carolina's CON laws frequently intrude into service areas that most other CON states leave untouched by their CON programs. For example, only half of the 25 health care services regulated by CON laws in North Carolina are also regulated by majorities of other CON states (see Table 1). Five services regulated by North Carolina's CON program — burn care (10 other CON states), CT scanners (12), renal failure/dialysis (11), subacute services (12), and assisted living and residential care facilities (only 4 other CON states) — are regulated in one-third or fewer of the other CON states.
With these factors in play, the Mercatus researchers saw "a particularly rich opportunity to reverse course and open the market for greater entry, more competition, and ultimately more options for those seeking care." I agree.





























