Publisher's note: The author of this post is Katherine Restrepo, who is the Health and Human Services Policy Analyst for the John Locke Foundation.
The excessive amount of government intervention that has been entrenched in our nation's health care system is curiously pushing medical providers to channel this negative energy into positive solutions — ones in which physicians are either scaling back or cutting off their relationships with middleman insurers to spend more time with their patients.
The business model is known as
direct primary care (DPC). In exchange for a monthly or annual fee that covers a defined package of services, patients have guaranteed unlimited access to their physicians. DPC is similar to concierge medicine, but the key difference is that these practices deliver basic health care at an affordable price with no insurance billing whatsoever.
In just a few weeks, direct primary care practice
Doctor Direct will be opening its doors here in Raleigh. The physician entrepreneur behind Doctor Direct, Dr. Amy Walsh, tells me that monthly fees range from $50-$85 for adults and are around $15 for children. In return, patients can schedule same-day appointments and access services including but not limited to comprehensive physicals, EKG testing, joint injections, laceration repairs, and skin biopsies. To top it off, her solo practice is allegedly the first among DPCs in the state to dispense prescription drugs in-house.
The beauty of practices like Doctor Direct is that the traditional doctor-patient relationship is restored. By cutting the
40 percent of overhead that is normally spent on getting paid by insurance companies, primary care providers can devote hour-long appointments to their patients and deliver care at a fraction of the cost. Just take a look at some of the negotiated discount prices for labs and medications Doctor Direct offers. Note that these charges are in addition to membership fees:
DPC has been around for years, but it's a growing market that continues to pique physician interest. As of 2014, over 4,400 doctors in the US had taken the plunge — a
significant increase from just 146 in 2005. You can check out a national directory
here:
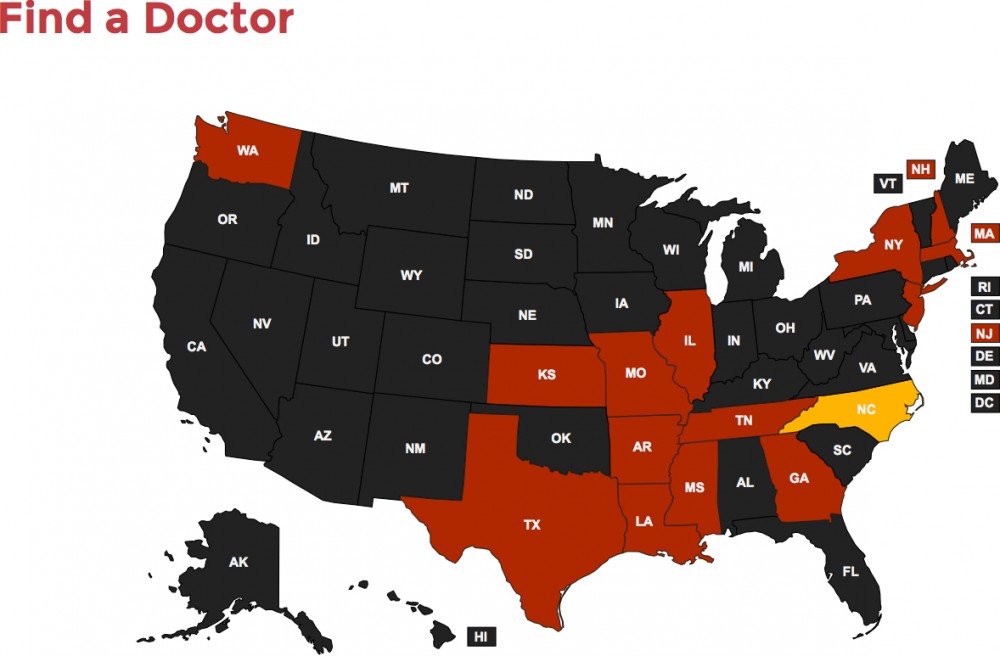
Fortunately, North Carolina ranks as one of the
top DPC-friendly states. Unlike other state legislatures, ours does not subject these practices to government price controls, capped patient numbers, or a defined menu of services. Some states even regulate these providers under the Department of Insurance (DOI) — the interpretation being that monthly cash payments to access medical care should be classified as insurance.
Since DPC typically does not deal with insurance, many may be wondering how it can thrive now that Obamacare requires individuals and employers to purchase government-approved health plans that cover preventative care. Interestingly, the federal health law
does endorse DPC as long as it is accompanied by catastrophic policies that include benefits outside of primary care.
So, if a patient purchases a "wraparound" plan in conjunction with seeking care through a DPC practice, the individual mandate is fulfilled.
The problem, however, is that most insurers have not taken the initiative to offer these types of plans, since DHHS Secretary Sylvia Mathews Burwell has yet to clarify what benefits must be included for them to be deemed as "qualified." In the meantime, it's recommended that patients who partake of direct care also purchase a high-deductible health plan for medical emergencies.
The other federal obstacle holding back the DPC floodgates is that Obamacare and the IRS currently don't
speak the same language on the issue. The law does NOT classify direct care payments as insurance, yet the IRS does. What this ultimately means is that patients cannot use pre-tax HSA funds to pay for monthly membership fees.
The good news is that
bipartisan legislation has been introduced in the US Senate to fix this discrepancy. All that is needed is a tweak in the internal revenue code to allow for these recurring fees to be recognized as any other tax-free medical expense. The bad news is that no one knows how long it will take for this to actually happen.
If and when these hurdles are cleared, this innovative health care delivery method will only continue to flourish more than it already is.